
Vertex Pharmaceuticals
Vertex took a bold step in developing a $10 billion-a-year drug for a rare yet life-threatening condition, disregarding conventional wisdom that there was no market for it. How did they succeed?


Vertex Pharmaceuticals is an American biotech company headquartered in Boston, Massachusetts. Vertex is most famous for developing novel Cystic Fibrosis (CF) drugs, a condition that only affects 100,000 worldwide, for which Vertex is now worth over $90 billion and is one of the 15 largest pharma companies in the world. Founded in 1989, the company took over 20 years and $4 billion of investors cash to become profitable. If not for its founder, it would not have gotten involved in researching the drugs for which it has become most famous.
While most pharmaceutical companies operate by designing marginal improvements to existing treatments, Vertex was founded to develop drugs for small target markets. When it was founded, this approach was unorthodox. Fortunately, it has been exceptionally financially lucrative and has massively benefited Cystic fibrosis sufferers while inspiring the creation of biotech companies invested in developing drugs for specific conditions. However, future genetic therapies may prove prohibitively expensive for healthcare providers, especially outside of the United States.
Early Years - Search for HIV Treatments
Vertex was founded by Joshua Boger and Kevin Kinsella. Kinsella was a venture capitalist who founded Avalon Ventures with a $400,000 loan from a friend in 1983. He went on to help found over 125 companies and was a producer on the musical Jersey Boys. Boger had graduated from Harvard in 1979 with a PhD in chemistry, then briefly worked with future Nobel prize winner Jean-Marie Lehn before joining Merck. Merck was a giant in the pharmaceutical industry with decades of breakthroughs. In the 1940s, Merck had developed the first antibiotic, penicillin. In the 1960s, Merck released lovastatin, the first statin drug used to lower cholesterol, and had then developed the constituent vaccines in the MMR vaccine. In the 1980s, Merck had a reputation for a better research environment than more profitable companies such as Pfizer, but this approach of working on groundbreaking research was gradually being changed by management. In part, this was due to many low-hanging pharmaceutical breakthroughs having all been eaten up, but also due to the more onerous safety regimes after the wake of the thalidomide scandal, and is also due to the incentives of the US healthcare system, where patients rarely pay the list price for medications and can ask for drugs with marginal benefits. Instead of developing new treatments for diseases, Merck executives wanted to pursue a more profitable and safer strategy to build on existing treatments and aggressively promote them to the healthcare industry.
In 1988, Boger ran an immunology team within Merck but was increasingly frustrated by management's approach. After his close friend within the company, Dr. Irving Sigal, who was running Merck AIDS research efforts, died in the Lockerbie bombing, Boger decided to leave and start his own company. Many early Vertex employees, like Boger, had previously worked at Merck. While Vertex initially didn’t hold any patents and the company didn’t produce any drugs, it was kept afloat by relying on investors, partnerships with universities, and larger companies to fund its research efforts. Although the company was not generating an income by 1993, it had raised over $50 million and had dozens of competitive research projects in rare diseases. One early success was a $20 million partnership with a Japanese company, Kissei Pharmaceuticals, to develop AIDs medications.

Vertex Founder Joshua Boger
Vertex started with the goal of developing small-molecule drugs to tackle diseases, underpinned by a broad research portfolio. Small molecule drugs are organic compounds utilized as therapeutic agents in medicine. These drugs are usually chemically synthesized, allowing them to permeate cell membranes and interact with target molecules inside cells. Most small-molecule drugs can be taken orally rather than being injected, making them far easier to administer. Importantly, once the compounds are discovered, the drugs can be manufactured for a fraction of their labeled cost.
Drug discovery is expensive and time-consuming. Before clinical trials can begin, the preclinical research stage to identify promising molecules that interact with the intended targets can prove fruitless. Even if a molecule is identified, companies may find it unsafe for human consumption in preclinical lab tests. Although estimates vary, on average, it takes over $1.3 billion to bring a drug to market, which start-up pharmaceutical companies will not usually be able to raise on their own. For genetic medicines, the cost is estimated to be far higher, averaging around $2 billion. Often, companies with promising research pipelines or drugs are acquired by larger pharma companies, sometimes cynically, if the smaller company has a drug that could significantly impact the larger companies' revenue stream. In 2017, Mallinckrodt Pharmaceuticals settled with the Federal Trade Commission after it was accused of violating anti-trust laws by buying a company that had previously acquired a competitor to its anti-inflammatory drug Achtar.
Five years after Boger founded the company, Vertex had not brought any drugs to market but was putting significant resources into developing drugs to help treat HIV/AIDS. By the mid-1990s, AIDS was killing tens of thousands of Americans a year, primarily gay men who had contracted the disease via sexual intercourse. While Zidovudine, also known as azidothymidine/AZT, an antiretroviral drug, had been introduced in 1987, it was not effective on its own. In the early 1990s, Vertex was working on a small molecule that aimed to bind itself to the active site of HIV proteases, which, in theory, would stop the replication of the virus as proteases, enzymes responsible for cleaving protein sections, enable HIV multiplication. Eventually, Vertex did release Agenerase in 1999, but larger companies, such as Merck and Roche, had beaten Vertex to it.
Miracle Hunting - Finding a treatment for Cystic Fibrosis
In the traditional approach to small-molecule drug development, researchers would discover small-molecule drugs primarily by screening extensive compound libraries against assumed biological targets. Researchers would search for "hits" based on characteristics like shape, electrical charge, and affinity for or aversion to water. Medicinal chemists would subsequently attempt to refine these properties through modification. Instead, Boger wanted to develop drugs using structure-based design, which required large amounts of computing power to model and simulate molecules interacting with proteins and enzymes.
Boger was also hunting for assays (lab tests designed to mimic diseases) to test the molecules Vertex had been developing against. Aurora Bioscience was a business founded to help larger companies develop drugs by developing assays for their particular interests, but it had decided to move towards drug development itself. In the early 2000s, Wall Street funding for pharmaceutical companies was scarce. As a part of its regular business, Aurora had an ongoing $300,000 contract with the Cystic Fibrosis Foundation (CFF), a US-based charity, to develop an assay for the disease. In search of more funding, Aurora had agreed to a $30 million contract with CFF to develop three drug candidates ready for the preclinical and clinical research stages to treat the underlying causes of CF, with funding only released if Aurora met strict milestones. In return for the investment, the CFF would receive royalties to any drugs released onto the market instead of equity in Aurora, keeping the incentives for both parties to develop effective drugs for patients firmly aligned. This method of funding was known as venture philanthropy.
Cystic fibrosis is a genetic condition in which mutations in the CFTR (cystic fibrosis transmembrane conductance regulator) gene can lead to cystic fibrosis (CF). The CFTR gene provides instructions for producing a protein that regulates the flow of chloride ions across cell membranes. These chloride ions are crucial in maintaining salt and water balance in various organs, including the lungs and digestive system.
Over 1800 different mutations can occur in the CFTR gene, each resulting in varying degrees of impairment in the function of the CFTR protein. However, most people with CF have a mutation called DF508, meaning if a treatment could be found for that mutation, it would be effective for tens of thousands of CF sufferers. The defective CFTR protein in the lungs produces thick, sticky mucus that is difficult to clear. Normally, airway epithelial cells produce a thin layer of mucus that helps trap and remove inhaled particles and bacteria. However, in individuals with CF, the abnormal mucus becomes dehydrated and accumulates in the airways, leading to obstruction, inflammation, and recurrent infections.
These infections would typically reduce the life expectancy of the sufferer to 31. While the genes responsible for the cruel life of the person afflicted had been discovered in 1989, there was only minimal progress in treatments. The day-to-day life of a person with CF included dozens of tablets with varying levels of unpleasant side effects and hours of chest physio to keep the disease at bay. Treatments and tablets were only able to delay inevitable inpatient hospital visits to administer round-the-clock intravenous antibiotics for a few weeks or months at a time. The late Claire Wineland documented years of her life, including her final days, showing the relentless cycle of treatments and illness Cystic Fibrosis inflicts without effective treatments.
When Vertex bought Aurora, it was not obligated to continue its partnership with the CFF. Boger said, “I knew that this cystic fibrosis assay work was being done, but frankly, it wasn’t even in the top 10 things we were interested in the company for”. The partnership could have ended in 2001. Boger was strongly encouraged to do this by almost everyone he spoke to about the partnership, but he had started Vertex in order to develop breakthrough drugs. He decided to stick to his convictions despite the small CF population and no clear way to profit from the endeavor. It would turn out to be an incredibly fortuitous decision.
In Boger's words, they had to make “a pill that would make a protein that’s not working work.”As a research proposition, it was “scary as hell.” Still, within the venture philanthropy framework, it did make sense to continue investigating, especially as the CFF was willing to provide the majority of funding.
Eric Olson, who led CF drug development at Vertex from 2001 to 2013, was the person tasked with making malfunctioning CFTR work. He became intrigued by the disease after working with a colleague whose daughter suffered from the condition, combating pseudomonas, the most prevalent bacterium that targets the lungs of CF patients. Olson's team began by aiming at the G511D mutation, which only 4% of CF patients carried. In 2005, at Vertex’s San Diego facility, they discovered that they could alter the functioning of the gene. Further results in 2008 showed a 10% improvement in lung function. After clinical trials confirmed this result, the Food and Drug Administration approved Kalydeco, the brand name for ivacaftor, in January 2012. Initially, Vertex priced this drug at $300,000. Although over a thousand patients were soon taking the drug, with many seeing significant increases in quality of life, this was still only a small percentage of the total number of CF patients. In 2014, the CFF, having seen their investment pay off and wanting to avoid any future conflict of interest, sold the rights to the royalties for the drugs Vertex had developed for over $3 billion. The venture philanthropy framework had worked to develop drugs treating the underlying cause of CF, and the profits for the CFF would see dozens of other projects funded.
Based on the positive rollout, Vertex was already working on follow-up drugs. In 2015, Orkambi was approved by the FDA, increasing the number of patients on a CFTR modulator in the US to just under 10,000. Orkmabi resulted from combining ivacaftor with a new compound, lumacaftor. In Britain, although some CF patients were taking the drug as a result of either their participation in clinical trials or due to compassionate use, a battle to get the drug approved for those with suitable genes was underway. Unlike the US, where insurers foot the bill for medical care, in the UK, the state pays for healthcare under a free-at-the-point-of-use system. To keep drug costs under control, the National Institute for Health and Care Excellence (NICE) reviews drugs under a cost-benefit analysis system. Theoretically, this thoroughly analyzes a drug's benefit to patients and the healthcare system versus its costs. Still, the analysis is constructed with assumptions about the efficiency of treatment using conventional methods and is implicitly constrained by the amount of money that taxation can raise. This meant that patients in the UK did not receive Orkambi until 2019, when Vertex was in the final stages of developing its most effective CF drug yet, Trikafta, targeting the DF508 mutation that most CF sufferers possessed. Like Orkambi, Trikafta is a combination therapy made from tezacaftor, ivacaftor, and elexacaftor.
Paying the Price - Patients vs Costs
Trikafta had sped through approval to get to patients. It received an expedited approval process, including Priority Review, Fast Track, Breakthrough Therapy, and orphan drug designation. In late 2019, Kaftrio was approved for prescription to tens of thousands of patients in the US. It was again priced at over $300,000 a year in the US, meaning every tablet of the three-pill-a-day regime (two taken in the morning with a third at night) cost $270.
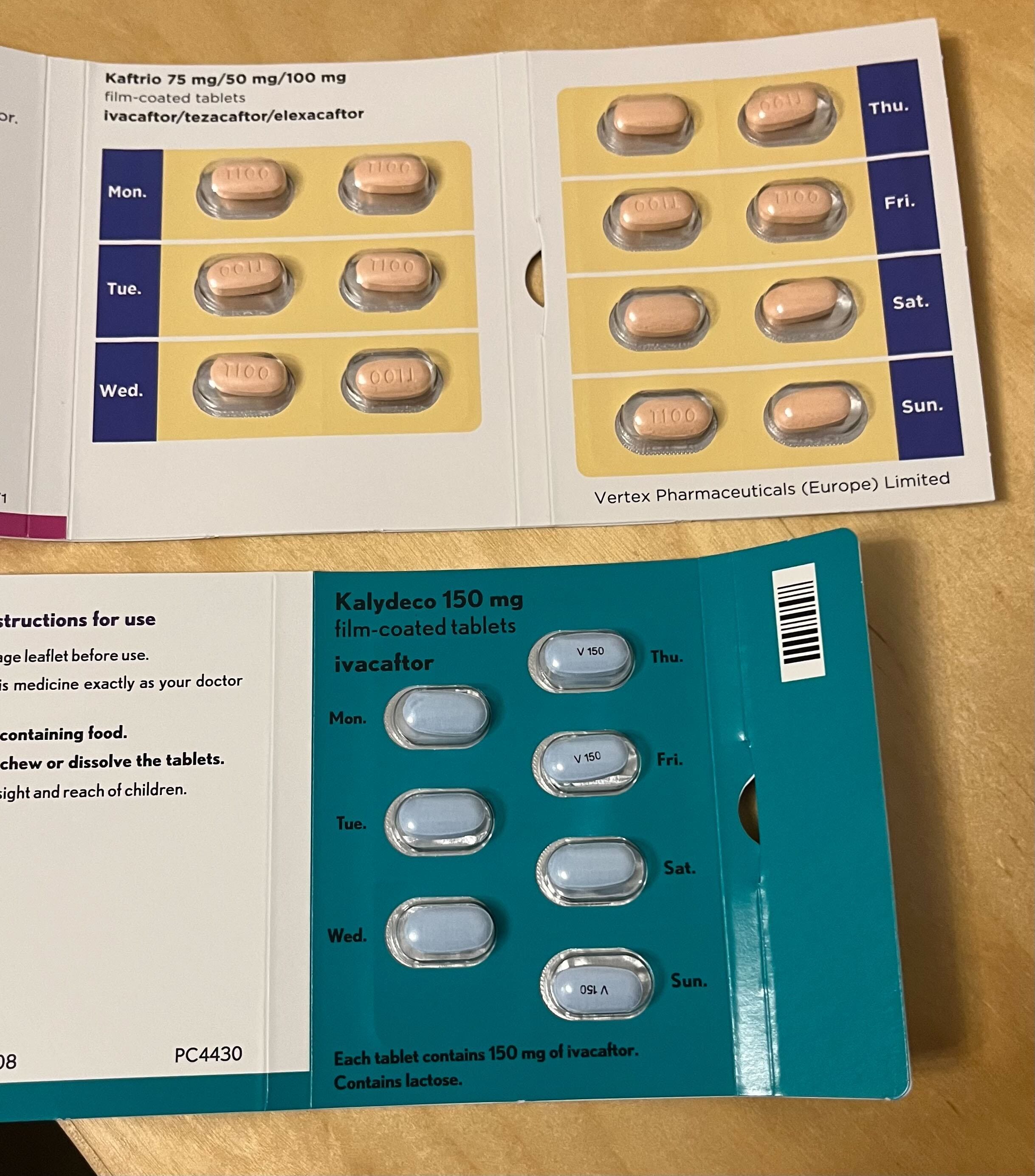
A week’s worth of Trikafta (known as Katrio in Europe) tablets. In the US, these tablets would cost $5670 without insurance coverage.
There was considerable excitement in the UK at the prospect of this revolutionary drug. Still, there was apprehension at how long it had taken Vertex and the NHS to agree on a price for Orkambi. NICE’s appraisals are commonly used by smaller countries that do not have the resources to conduct analysis by themselves, a fact known by NICE, which means they are not just setting NHS prices but also drug prices in other European countries. The pricing battle between Vertex and British authorities had led to a darkly comical situation in which thousands of packs of drugs had been destroyed rather than distributed to patients in need.
However, in late 2019, another medical development was underway to change the lives of many more people than the CF population. As COVID-19 began to spread worldwide, an unseen effect of the huge amounts of money spent to support economies worldwide was the massive price tag of Kaftrio suddenly seemed insignificant. Against the advice of NICE, the NHS and Vertex agreed on a price for Trikafta in 2020. Patients in the UK began receiving the drug in August.
Although some details of the agreement were kept secret, it has been reported the NHS managed to get the cost down to $200,000. One detail that wasn’t secret was that NICE would review the cost over a four-year period. In 2023, NICE released its initial report claiming that despite the drug being effective, Trikafta was not cost-effective and that any future patients who were not previously eligible would not receive the drug. The NHS was paying hundreds of millions a year to Vertex for Trikafta. Supporters of continuing access pointed out that the cost of admitting patients with chest infections had fallen massively, freeing up desperately needed hospital beds, and continued access to the drug would mean the most expensive clinical interventions, such as lung transplants (which can cost over $5 million per patient) would also fall, as well as patients having much longer lifespans. NICE disregarded these arguments.
To campaigners for cheaper drugs for access outside of the US and richer countries with one-off agreements, the cost of manufacturing drugs is a disgrace. Trikafta is estimated to cost $5,676 for a year's treatment in manufacturing and packaging, while the drug is sold in the US for $300,000. Vertex claims they invested over $10 billion in R+D to develop the drugs, although they are unclear if this is specific to CF. Finding a balance between development costs and access is a deeply emotionally charged issue.
Unusually, the cost of Trikafta was even causing issues in the US. States such as Washington, Oregon, Colorado, Maryland, and Minnesota have looked into capping the amount that Vertex and other drug companies can charge for treatments, which may cause companies to withdraw from those markets. Patients with CF could be denied access to the life-changing drug and return to a future full of hospital admissions and shortened lifespans. This problem of life-changing medicines versus unsustainable costs will continue to affect those on the hook for the bill. The pharmaceutical industry, while appearing cruel by limiting access to treatments through high prices, incentivizes further drug development. When Orkambi was the leading treatment for CF patients with only one copy of the DF508 gene, analysts predicted it would earn over $20 billion from the lifetime of the drug. Within four years, it had released Kaftrio, sending the price of Okrambi from $300,000 to under $30,000, demolishing its own revenue stream.
The Future of Vertex
Ultimately, the patents on Kaftrio will expire in 2037, and the company will need new drugs to continue its profitability. Vertex now has many drugs in its pipeline to treat various diseases, including sickle cell disease, beta-thalassemia, Duchenne muscular dystrophy, alpha-1 antitrypsin deficiency, pain, and APOL1-mediated kidney diseases. The company's genetic modulator for sickle cell may cost as much as $2.2 million per patient.
One promising breakthrough drug is Vertex’s pain medication. Typically, opioids are used to manage pain relief resulting from surgery or injury, and drugs such as OxyContin work by binding themselves to opioid receptors in the nervous system, which blocks pain but also interferes with the brain’s reward system, leading to addiction if the dosage is not closely monitored. Millions of Americans have died due to becoming addicted to opioids and turning to heroin or fentanyl once prescription medications become unavailable to them. It is estimated that 10 million Americans are addicted to opioids. VX-548 is a new class of pain medication designed to prevent receptors in neurons outside the brain from detecting painful stimuli. Vertex is optimistic that VX-548 will not have the addictive properties of opioids and will be a profitable asset for the company.
For CF patients, Vertex continues developing drugs to increase lung function and adherence. Vanza, the successor drug to Trikafta, is due to be released in the US in late 2024, taking the three-pill regime down to a single pill with a modest increase in lung function over Trikafta. How popular this drug will be is an open question. Patients can only take Trikafta or Vanza, and it would appear Vanza is at either risk of cannibalizing Vertex’s Trikafta businesses or not being deemed beneficial enough to switch patients over from Trikafta, which seems to be the likely conclusion of NICE which doesn’t want to pay for Trikafta anyway. However, Vanza has been developed without needing to pay the full royalties concerning the agreement signed by the CFF over 20 years ago. Short of a cure, there may only be marginal gains from further CFTR modulators, but Vertex is intent on making the most of its remaining patent and scientific advantage.
Conclusion
Vertex is earning $9.87 billion a year from its CF treatments. It has created a breakthrough treatment and extended patients' lives by decades. They are currently working on a cure for CF delivered based on their breakthrough treatment, which, if successful, will destroy their current revenue stream from their most advanced CFTR modulators, just as they previously did with Okrambi by developing Trikafta. If healthcare systems refuse to pay for these kinds of therapies, it is not just the specific patients of treatments already in development who will suffer. The massive amounts of money Vertex has earned have spurned the creation of several companies and research efforts to alleviate or cure other conditions. While it remains to be seen if Vertex can actually pull off a cure for CF, which would require permanently altering the CFTR to function properly, its track record so far suggests it is earnestly pursuing this goal. Such a discovery would not be entirely selfless, as it would make the company tens if not hundreds of billions of dollars, but this revenue could fund decades of research into other genetic diseases, bringing genuinely miraculous cures to potentially millions of people around the world.
While the pharmaceutical industry’s reputation has suffered due to pricing scandals since Boger founded Vertex in 1989, technology has raced that many previously untreatable conditions now look conceivably treatable or curable. The American healthcare system is horrendously expensive for Americans, but it clearly spurs innovations that benefit the rest of the world. Whether Americans will continue to pay this cost remains to be seen. With a strengthening US economy, versus Europe in particular, treatments may be out of reach for patients worldwide. Some countries will deny patients access to these treatments, while others will seek to remove patent protections on drugs to treat their own citizens. A lesson for patients is that perhaps to receive access to innovative drugs, participation in clinical trials may allow them to continue receiving effective drugs even if the healthcare systems in their countries refuse to pay for them. Vertex may have inadvertently set the pieces in place to disrupt the global pharmaceutical industry truly, but perhaps not in the way they intended.
There are still people who are not eligible for the drugs that have changed the lives of so many people with Cystic Fibrosis. If you enjoyed this edition of the Kitstack, please consider donating to the Cystic Fibrosis Foundation (US) or Cystic Fibrosis Trust (UK) as they continue to do marvelous work supporting people with Cystic Fibrosis, particularly those who are not eligible for current treatments.